Drug Interaction Risk Calculator
How your body processes medications
Based on the article about pharmacokinetics, this tool calculates your risk of drug interactions considering key factors that affect how your body processes medications.
Your Risk Factors
Ever wonder why one person takes a pill and feels fine, while another gets dizzy, nauseous, or even ends up in the hospital? It’s not luck. It’s not magic. It’s pharmacokinetics - the science of how your body handles drugs. This isn’t just something pharmacologists talk about in labs. It’s the reason your doctor adjusts your dose, checks your kidney function, or warns you not to drink grapefruit juice with your medication. Understanding how your body absorbs, distributes, metabolizes, and excretes drugs isn’t just academic - it’s the key to avoiding dangerous side effects.
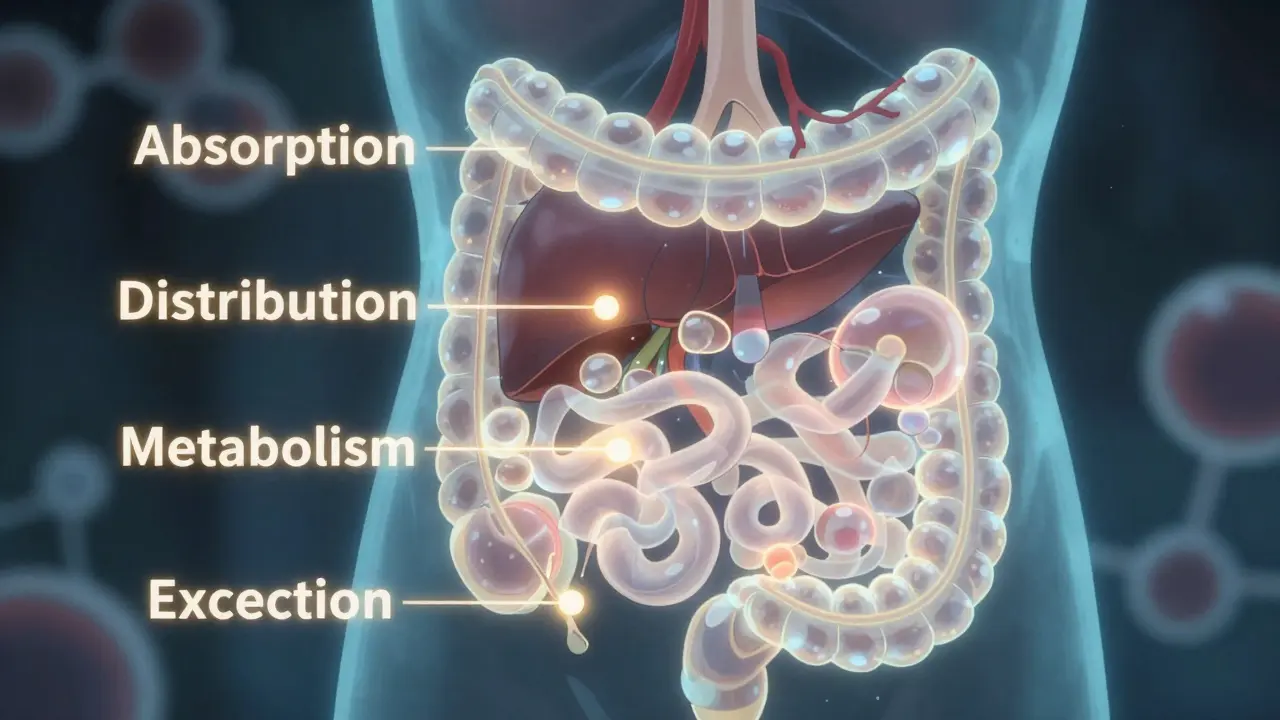
What Happens When You Take a Pill? The ADME Cycle
When you swallow a pill, inject a drug, or apply a patch, your body doesn’t just accept it. It processes it in four clear steps, known as ADME: Absorption, Distribution, Metabolism, and Excretion. These aren’t random events. Each step has measurable rules, and when they go off track, side effects happen.
Absorption is how the drug gets into your bloodstream. Oral drugs don’t just dissolve and vanish. They must pass through your gut lining. About 95% of drugs get in through passive diffusion - meaning they move naturally from high to low concentration. But factors like stomach acid, gut speed, and even your gut bacteria can block or boost this. For example, if you take an antibiotic with food, absorption might drop by half. Or if you’re on a drug like digoxin, a protein called P-glycoprotein can push the drug back out of your gut, cutting absorption by 30-70%. That’s why some meds must be taken on an empty stomach.
Distribution is where the drug travels after entering your blood. Not all drugs go everywhere. Some stick tightly to proteins in your plasma, like warfarin, which is 98% bound to albumin. That means only 2% is free to work - and that tiny amount is what affects your blood thinning. If another drug displaces warfarin from those proteins, that 2% can suddenly jump to 5%, causing dangerous bleeding. Other drugs, like antidepressants, soak into fatty tissues and linger for days. This is why some side effects appear days after you start a new pill.
Metabolism: The Body’s Drug Factory
Your liver is the main drug factory. It uses enzymes - mostly from the CYP450 family - to break down drugs into metabolites. CYP3A4 alone handles half of all prescription drugs. But here’s the catch: your enzymes aren’t the same as your neighbor’s. Genetics play a huge role. About 3-10% of Caucasians have a variant in CYP2D6 that makes them poor metabolizers. That means codeine, which needs to be turned into morphine by this enzyme, won’t work for them. On the flip side, some people are ultra-rapid metabolizers - they turn codeine into morphine too fast, risking overdose even at normal doses.
Drug interactions are another major player. If you take clarithromycin (an antibiotic) with simvastatin (a cholesterol drug), the antibiotic blocks CYP3A4. Simvastatin levels can spike 10-fold. That’s not a small increase. It raises your risk of rhabdomyolysis - a condition that breaks down muscle and can kill your kidneys. This kind of interaction causes 20-30% of serious drug side effects.
Excretion: Getting Rid of the Rest
Your kidneys clear about 80% of drugs. That’s why doctors check your creatinine levels before prescribing. Normal kidney function filters 90-120 mL of blood per minute. But if you’re over 65, have diabetes, or are on dialysis, that number can drop below 15. If your doctor doesn’t adjust your dose, drugs like vancomycin or metformin build up. One Reddit user shared a case: a 78-year-old woman on standard vancomycin doses developed kidney failure because her reduced clearance wasn’t accounted for. Her creatinine jumped from 1.2 to 3.4 in just a week. That’s preventable.
Some drugs are excreted in bile and reabsorbed - a cycle called enterohepatic recirculation. This is why some drugs, like diazepam, have effects that last for days. Its main metabolite, desmethyldiazepam, has a 100-hour half-life. In older adults with slower metabolism, this builds up, causing confusion, falls, and memory problems. That’s not just aging - it’s pharmacokinetics.
Why Side Effects Aren’t Random - They’re Predictable
Side effects aren’t accidents. They’re often the direct result of drug levels going too high. Take phenytoin, an old epilepsy drug. At therapeutic levels (10-20 mcg/mL), it controls seizures. Above 20 mcg/mL, toxicity kicks in: tremors, slurred speech, even coma. Studies show 30% of patients with levels over 20 have toxicity. Only 2% do at normal levels. That’s a 15-fold difference. It’s not about being "sensitive" - it’s about pharmacokinetics.
Age changes everything. People over 65 have 30-50% less liver metabolism and 30-40% lower kidney clearance. That’s why they’re three times more likely to have bad reactions. It’s not that they’re weak - it’s that their bodies process drugs slower. Yet, most prescriptions still use standard adult doses.
Genetics matter too. Warfarin, a blood thinner, has a very narrow safety window. A single gene variant in CYP2C9 can make someone 5 times more likely to bleed on a standard dose. That’s why genetic testing is now recommended before starting warfarin - and why some clinics test for it routinely.
Real-World Mistakes and How to Avoid Them
Doctors and pharmacists aren’t ignoring pharmacokinetics. But the system is messy. A 2022 Mayo Clinic survey found that 42% of patients who had bad reactions had at least one known risk factor - age, kidney disease, or multiple drugs - that wasn’t addressed when the drug was prescribed.
Here are three common mistakes:
- Dosing by weight alone - Many drugs are dosed by body weight, but if you’re over 65, your metabolism is slower. A 70kg 70-year-old needs less than a 70kg 30-year-old.
- Ignoring drug interactions - OTC meds like ibuprofen or antacids can interfere with absorption. Even St. John’s Wort, a natural supplement, can reduce the effectiveness of birth control, antidepressants, and blood thinners.
- Not timing levels correctly - Therapeutic drug monitoring requires drawing blood right before the next dose (trough level). If the lab draws it 2 hours late, the level looks lower than it really is. That can lead to dangerous overdosing.
Tools are improving. The FDA approved DoseMeRx in 2021 - an AI tool that cuts vancomycin dosing errors by 62%. The European Medicines Agency launched PK4All in 2023 to build better models for rare diseases. And the NIH just funded $185 million to study pharmacokinetics in diverse populations - because 85% of past studies were done on young, white men, even though they make up only 15% of drug users.
What You Can Do
You don’t need to be a scientist to protect yourself. Here’s what helps:
- Always tell your doctor or pharmacist about everything you take - supplements, vitamins, even herbal teas.
- Ask: "Is this dose right for my age and kidney function?"
- If you’re on a drug with a narrow window (like warfarin, lithium, or phenytoin), ask if therapeutic drug monitoring is needed.
- Don’t assume "natural" means safe. Grapefruit juice can raise blood pressure meds by 300%. St. John’s Wort can make birth control fail.
- If you feel off after starting a new drug - dizziness, nausea, confusion - don’t brush it off. It might not be "just side effects." It might be a buildup.
Pharmacokinetics isn’t about fear. It’s about control. When you understand how your body moves drugs, you can work with your doctor to find the dose that works for you - not just the one that works for the average person. That’s the future of medicine: not one-size-fits-all, but one-size-fits-you.
What does pharmacokinetics mean?
Pharmacokinetics is the study of how your body processes a drug - specifically how it absorbs, distributes, metabolizes, and excretes it. It’s often summed up as "what your body does to the drug," in contrast to pharmacodynamics, which is "what the drug does to your body." This science helps predict how much of a drug stays in your system and for how long, which directly affects its effectiveness and safety.
Why do some people have worse side effects than others?
Differences in side effects come from variations in pharmacokinetics. Factors like age, genetics, kidney and liver function, and other medications all change how a drug is handled. For example, people with a CYP2D6 gene variant may not convert codeine into its active form, making it useless. Others may metabolize it too quickly, leading to overdose. Older adults often have slower metabolism and reduced kidney clearance, so drugs build up. Even something as simple as eating grapefruit can block drug breakdown and cause dangerous spikes in blood levels.
Can diet affect how drugs work?
Yes, diet can have a major impact. Grapefruit juice blocks the CYP3A4 enzyme in your gut, which can cause drugs like simvastatin or felodipine to build up to toxic levels. High-fiber diets can slow absorption of some antibiotics. Calcium-rich foods can bind to tetracycline antibiotics, preventing absorption. Even a simple change like taking a pill with food instead of on an empty stomach can cut absorption in half for certain drugs. Always check if your medication has dietary restrictions.
How do doctors know if a drug dose is right for me?
For some drugs, doctors use therapeutic drug monitoring (TDM), which measures the drug level in your blood. This is common for drugs like warfarin, lithium, phenytoin, and vancomycin. They look at both peak and trough levels - the highest and lowest concentrations between doses. They also consider your age, weight, kidney and liver function, and other medications. Newer tools use AI models to predict the best dose based on your profile, reducing guesswork and lowering the risk of side effects.
Are generic drugs processed the same way as brand-name drugs?
Generic drugs must contain the same active ingredient and meet strict bioequivalence standards - meaning they deliver the same amount of drug into your bloodstream as the brand name. However, inactive ingredients (like fillers or coatings) can differ. These can affect how quickly the drug is absorbed, especially for drugs with a narrow therapeutic window. For most people, generics are safe. But if you’ve had side effects or poor response with a brand-name drug, switching to a generic might require monitoring - especially for epilepsy, thyroid, or blood thinner medications.