When you pick up a prescription and see a generic version instead of the brand-name drug you recognize, it’s natural to wonder: Does this really work the same? The answer lies in bioequivalence testing - a rigorous, science-backed process that ensures generic drugs deliver the same results as their brand-name counterparts. This isn’t marketing. It’s regulatory science. And it’s why over 90% of prescriptions in the U.S. are filled with generics - without compromising safety or effectiveness.
What Bioequivalence Testing Actually Measures
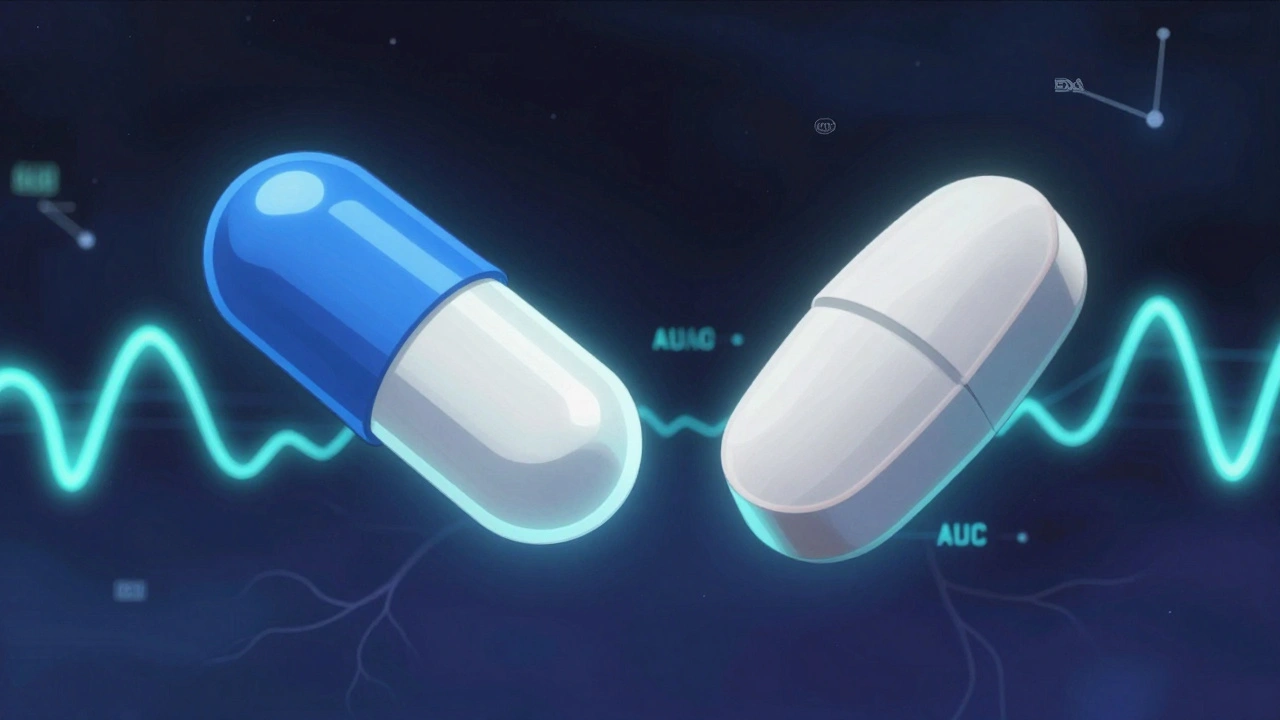
Bioequivalence testing doesn’t ask whether a drug cures the same disease. That’s already proven by the brand-name version. Instead, it asks: Does the generic drug get into your bloodstream the same way, at the same speed, and in the same amount? The answer is measured through two key numbers: AUC (area under the concentration-time curve) and Cmax (maximum concentration in the blood).
For a generic drug to be approved, its AUC and Cmax must fall within 80% to 125% of the brand-name drug’s values. That’s not a guess. It’s a strict statistical range set by the FDA and accepted globally by the EMA, Health Canada, and other major regulators. If a generic drug’s AUC is 79% or 126%, it’s rejected. No exceptions.
These numbers come from studies with 24 to 36 healthy volunteers. Each person takes both the brand and generic versions - sometimes one first, sometimes the other - in a crossover design. Blood is drawn over hours to map how the drug moves through the body. The goal? Prove that the generic doesn’t just look like the brand - it behaves like it.
Why This Matters More Than You Think
Think of bioequivalence like a fuel injection system in a car. Two engines can have the same horsepower, but if one gets fuel slower or in smaller bursts, performance suffers. The same applies to drugs. If a generic drug is absorbed too slowly, it might not reach therapeutic levels fast enough. If it spikes too high, it could cause side effects.
For most medications - like antibiotics, blood pressure pills, or antidepressants - this 80%-125% window is more than enough. But for drugs with a narrow therapeutic index - where the difference between an effective dose and a toxic one is tiny - regulators demand tighter control. Drugs like warfarin, levothyroxine, and phenytoin require extra scrutiny. In some cases, the FDA requires additional studies or even clinical endpoint trials to confirm safety.
How Generic Drugs Are Approved (Without Repeating Clinical Trials)
Brand-name drugs go through years of testing: Phase I (safety), Phase II (dosing), Phase III (effectiveness in thousands of patients). That costs billions. Generics don’t repeat that. Instead, they use the Abbreviated New Drug Application (ANDA) pathway, created by the Hatch-Waxman Act in 1984.
Here’s how it works:
- The generic must contain the same active ingredient, strength, dosage form, and route of administration as the brand.
- It must be pharmaceutically equivalent - meaning it has the same ingredients, just possibly different fillers or coatings.
- It must pass bioequivalence testing.
- Its manufacturing must meet the same Good Manufacturing Practices (GMP) as the brand.
The FDA doesn’t need to retest whether the drug treats high blood pressure or diabetes. That’s already proven. They only need to prove the generic delivers the drug the same way. This cuts approval time from 10+ years to about 10 months and saves the U.S. healthcare system over $300 billion a year.

What Bioequivalence Testing Doesn’t Prove
It’s important to know what this test doesn’t cover. Bioequivalence focuses on systemic exposure - how much drug reaches the bloodstream. It doesn’t guarantee identical results for drugs that act locally.
For example:
- Inhalers: You can’t measure drug concentration in the lungs with a blood test. The FDA now requires clinical endpoint studies - like measuring lung function - to prove equivalence.
- Topical creams: Absorption through the skin varies based on application technique, skin thickness, and formulation. The FDA issued specific guidance in 2019 requiring in vivo bioequivalence studies for dermatological products.
- Extended-release tablets: These are designed to release drug slowly. A single bioequivalence study under fasting conditions isn’t enough. Regulators now require testing under fed conditions and sometimes multiple studies to cover different release profiles.
These exceptions aren’t loopholes. They’re science-driven updates to ensure safety where traditional methods fall short.
Real-World Evidence: Do Generics Work?
Numbers don’t lie. In a 2022 Consumer Reports survey of 1,200 people using prescription drugs, 87% reported no difference in effectiveness between their generic and brand-name versions. Nine percent even said the generic worked better. Only 4% felt the generic was less effective.
On Reddit’s r/pharmacy, over 1,400 users shared experiences. Most negative stories weren’t about the drug failing - they were about side effects from inactive ingredients. A different dye, filler, or coating can cause stomach upset or allergic reactions in sensitive people. But that’s not a bioequivalence failure. It’s an individual sensitivity. And it’s why pharmacists can swap brands if a patient reacts poorly.
Still, myths persist. A 2021 study found 32% of patients believe generics are less potent. That’s not science - it’s perception. The FDA’s Orange Book lists every approved generic and rates it for therapeutic equivalence. If it’s rated “AB,” it’s interchangeable. No exceptions.
Global Standards and the Future of Testing
The U.S., EU, Japan, Canada, and Australia all follow harmonized bioequivalence standards through the International Council for Harmonisation (ICH). Minor differences exist - for example, the EMA sometimes requires fed-state testing for certain drugs - but the core 80%-125% rule is universal.
What’s changing? Technology. The FDA is moving toward model-informed drug development. Instead of testing every generic in 30 people, scientists use computer models based on real-world data to predict how a drug will behave. This is already being used for complex generics like inhalers and injectables. The goal isn’t to cut corners - it’s to make testing smarter and faster without sacrificing accuracy.
By 2030, the global generic drug market is expected to hit $781 billion. That growth depends on trust. And trust comes from science - not slogans.
What You Should Know Before Taking a Generic
If your doctor prescribes a brand-name drug and you’re considering switching to generic:
- Ask if it’s rated “AB” in the FDA’s Orange Book. If yes, it’s interchangeable.
- Don’t assume a cheaper generic is less effective. The price difference is usually just packaging and marketing.
- If you notice a change in how you feel after switching, talk to your pharmacist. It might be the inactive ingredients, not the active one.
- For critical medications like thyroid drugs or blood thinners, stick with the same generic brand if you’ve found one that works - consistency matters more than cost.
There’s no magic in the brand name. The pill in the blue bottle and the one in the white bottle are chemically identical. The difference is in the cost - and the trust you place in the science behind it.
Is a generic drug just a copy of the brand-name drug?
Yes, but only in the active ingredient. Generics must contain the same active chemical compound, strength, dosage form, and route of administration as the brand. However, they can differ in inactive ingredients like fillers, dyes, or coatings. These differences don’t affect how the drug works - but they can sometimes cause minor side effects in sensitive individuals.
Do generic drugs take longer to work than brand-name drugs?
No. Bioequivalence testing requires that the generic reaches the same maximum concentration in the blood (Cmax) and stays there for the same duration (AUC) as the brand. If a generic took longer to work, it would fail the test and be rejected by the FDA. Any perceived delay is usually psychological or due to differences in pill size or coating.
Are all generic drugs the same?
All FDA-approved generics must meet the same bioequivalence standards, so they’re equally effective. But different manufacturers may produce different versions. If you switch between generic brands and notice a change in how you feel - even slightly - talk to your pharmacist. You may need to stick with one manufacturer’s version for consistency, especially with narrow therapeutic index drugs.
Why do generic drugs look different from brand-name drugs?
By law, generic drugs can’t look identical to the brand-name version - that would be trademark infringement. So they may differ in color, shape, size, or flavor. These changes are only in the inactive ingredients and don’t affect how the drug works. The active ingredient is identical.
Can I trust a generic drug approved by the FDA?
Yes. The FDA requires the same quality, strength, purity, and stability standards for generics as for brand-name drugs. Every generic manufacturer is inspected annually, and their facilities must meet the same Good Manufacturing Practices (GMP) as Pfizer, Merck, or any other brand. Over 90% of U.S. prescriptions are filled with generics because they’re proven safe and effective.
Are there any drugs where generics aren’t recommended?
For most drugs, generics are perfectly safe and effective. However, for drugs with a narrow therapeutic index - like warfarin, levothyroxine, or cyclosporine - doctors may recommend sticking with one brand (generic or brand-name) for consistency. This isn’t because generics are less effective, but because small changes in blood levels can matter. Always follow your doctor’s advice.










